
Increasing Effectiveness of Primary Prevention to Decrease Growth Rate of Health Care Costs
A Commentary on the Current Status of Healthcare in America
to download full pdf, click here
The Ongoing Problem of Health Care Costs in the U.S.
Health care spending for the United States is estimated to rise to $3.08 trillion in 2014, equating to about a 6.1% increase from last year.1,2,3,4 This staggering number overshadows that of other industrialized countries, even though our nation does not provide “objectively better access to care or quality of care.”2,5
Current trending topics celebrate the slow growth rate exhibited within the last 4 years, averaging just 3.7% annually. This number is historically lower than it has ever been (6.3% average between 1991 and 2011), but the fact of the matter is: numbers don’t lie and growth still means spending more.1,2,5,6,7,8 And despite various successful efforts to reduce this increasing trend in spending (i.e. the Affordable Care Act, new service delivery models7,8) CMS estimates the rate to once again rise to an average of 6.2% annually, from 2015-2022.1 This amounts to the U.S. spending approximately $5 trillion of its economy by the year 2022.
More effective measures need to be set in place to not just curb this growth rate but to reverse it.
Causes for the Continued Growth of Health Care Spending
There are multiple reasons that contribute to this continuing upward trend in health care spending, and these include hospital cost increases, hiking of prescription drug prices, provider prices, provider consolidation, high cost of insurance administration, increase in use of expensive medical technology, and many others.2,4,7,9 This article, however, chooses to address the source of health care provision: patient health.
One of the driving forces of health care costs is the constant battle with chronic disease. The burden of chronic disease continues to plague our health care system, with heart disease being the leading cause of death and one of the costliest health problems in the U.S.10 Researchers predict a 42% increase of chronic disease prevalance by 2023.11 This amounts to an additional $4.2 trillion spent in treatment costs and lost economic output.11 The missed opportunity with chronic disease is that most of the costs can be preventable, as risk factors for these conditions are mostly linked to unhealthy lifestyles.11 Obesity for example, a risk factor for heart disease, accounts for about 12% of the spending growth these past years.2,12 Preventing obesity and other risk factors can, therefore, save the U.S. economy by reducing health care money used to treat these chronic diseases. “The rising rate of chronic disease is a crucial but frequently ignored contributor to growth in medical expenditures.”11
Primary Prevention as a Solution
Primary prevention is an aspect of medicine that aims to reduce or prevent risk factors by modifying behaviors, specifically promoting a positive lifestyle, which includes nutrition and exercise.
Prevention has long been a part of the debate on ways to reduce health care spending, with both sides providing arguments to support their cases. Economist Louise Russell argued that prevention rarely reduces costs13, and researchers would say that prevention is no more cost effective than conventional medicine14, or that primary prevention has the “lowest potential” for cost savings among policy options.15 They argue that increasing screenings and tests to find one unhealthy patient among thousands of perfectly healthy individuals does not amount to positive savings.16
On the other hand, many healthcare and public health professionals continue to advocate primary care, and argue that primary prevention has short term, intermediate and long term benefits to both health and health care costs.17 Many supporters of primary prevention argue that at least one-third of ED visits are “avoidable” and could have instead been prevented through primary care settings, thus subtracting from the billions of dollars wasted annually from these “avoidable” ED visits.18 Dr. Jade Hiramoto of UCSF, recently stated that early detection and prevention of peripheral arterial disease in women could have decreased various risks that potentially could increase health care costs through various procedures, such as amputation and treatment.19
Both sides of the argument provide valid points, which is why researchers from the Partnership of Prevention and Robert Wood Johnson Foundation did extensive studies on the actual cost savings and cost effectiveness of primary prevention, where cost savings and cost effectiveness are defined as preventive care that decreases cost and preventive care that has benefits significantly larger than the costs, respectively. Both studies concluded that there are various preventive care services that are cost effective and provide cost savings, and successful implementation of preventive care as a reduction tool of health care spending requires the government to shift towards strategies that are low-cost yet highly effective.20,21
Our Strategies to Increase Effective Prevention at a Low Cost
Patient Commitment
This practice, over the years, has shown that primary care does not have to be expensive and our patients, with their commitment and the information shared by the office, want to get better and do strive to make these changes, thus increasing the effectiveness of the health care received.
Patient commitment is therefore a strong factor into making sure that patients stay on track with their health and positive lifestyle choices, thus minimizing hospital visits, intake of prescription medications, necessitating various expensive procedures and overall health care cost per quality-adjusted life years. These are evident in the graph below which is taken from a physician performance report done by Blue Shield of California on the practice in comparison to other physicians within the same specialty.33
Utilization Variation from Peers by Service Category
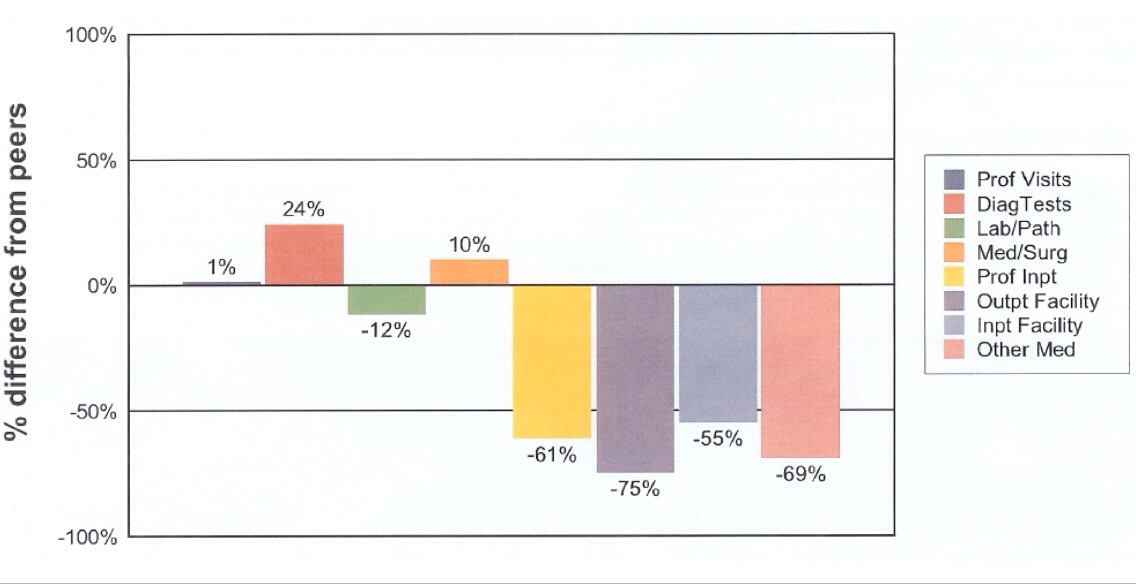
As can be interpreted from this graph, this practice and its patients uses 75% less Outpatient Facility procedures (-75%) than other practices and their patients, 61% less Professional Inpatient (-61%), 55% less Inpatient Facility (-55%) and 12% less Laboratory/Pathology (-12%). On the other end of that spectrum, the practice has a utilization percentage of 24% above others in Diagnostic Tests and 10% more for Medical and Surgical Procedures.
Vascular Doppler Waveform Analysis and Biofeedback Principles36,37
One of the ways the office helps motivate our patients with this commitment is to perform vascular evaluations as a means of biofeedback. The test, which analyzes the elasticity of a patient’s arteries through waveforms, provides them with real time insight into their arterial function and degree of plaque formation.22 More importantly, the test allows the patients to understand that atherosclerosis can be prevented or reversed, therefore decreasing the risk of disease, including heart attack, stroke, and other ailments. Subsequent tests can promote the positive lifestyle changes recommended for the patients by seeing improvement in their vascular waveforms, which are apparent in mere weeks.23,24,25
The effectiveness of this procedure in health improvement and cost savings is demonstrated in our case study on patient who avoided spending thousands of dollars on hospital bills and various procedures (i.e. by-pass surgery, coronary angioplasty and coronary angiograms) for her acute coronary syndrome by participating in our lifestyle modification program and repetitive Vascular Doppler analysis for more modest costs.34
The actual procedure of the Vascular Analysis is simple, non-invasive, non-time consuming,26 and applicable to youth and early prevention, as demonstrated in our research project: Vascular Improvement for Performance in Sports.35
Insurance Provider Involvement in Primary Prevention
Another strategy to increase effectiveness of primary prevention in reducing health care costs is to engage insurance companies, whether they are private or government funded.
Both types of payers have limited coverage for preventive services, despite their proven benefits, and yet they continue to reimburse various therapeutic services, despite the cost and lack of evidence of effectiveness. Insurance companies need to treat preventive procedures as they do therapeutic procedures, to give primary prevention a boost in effectiveness.20
As previously mentioned, insurance companies (i.e. Blue Shield) also have the capacity to evaluate physician performance. The office believes that the use of this information is probably being misused; and agrees with Ms. Debra Draper that there is a lot of missed potential with these studies in supporting positive performance by physicians. Meaningful incentives must be provided with these reports to physicians that exhibit good results, especially those that show effective prevention methods.27
Turning the tide on physician evaluations, the office also believes that the insurance companies and other agencies have the capability of showing patient performance. For example: blood pressure improvement, weight loss, decrease in the use of medication, or complete discontinuing of medications because of successful lifestyle improvement programs. Providing performance reports and meaningful incentives to patients that show improvement and commitment to better health should help with increasing the effectiveness of primary prevention.
Reduce Primary Care Physician Shortage
The final strategy to increase effectiveness of primary prevention suggested by this office is to reduce the dilemma of primary care physician shortage. According to multiple studies, the number of physicians interested in primary care has decreased significantly while the interest in specialties continue to increase.28,29 Increasing accessibility to primary care is important because studies show that quality primary care is associated with better health status and lower health care costs.
A study done by Dr. Christine Sinsky associates this decline to physician burnout, which other studies link to a decline in patient outcomes.30,31 Dr. Sinsky suggests that various innovations, including proactive planned care, shared care system, medical assistant order entry, and improved team communication can help lower the risk of physician burnout, all of which are exhibited by this office.32 Another important innovation to reduce burnout, which this office continually practices, is to have a strong patient-physician relationship and an increased responsibility and commitment of the patient.
Application of these innovations will successfully reduce risk of burnout, and will therefore increase patient income, increase interest in primary care, and drive forward the effectiveness of primary prevention.
Conclusion
The continued growth of health care spending has sparked the need for changes within our system. Various innovations have been presented, but this office chooses to focus on the primordial aspects of health care, and that is prevention of chronic diseases.
The role of primary prevention in reducing health care costs has been a topic of debate for years, however studies have shown that prevention is an important driving factor when cost effectiveness is apparent.
This office proposes strategies currently applied in this practice, that improve cost effectiveness of primary prevention and they include:
- Increasing patient commitment
- Use of vascular Doppler analysis and biofeedback principles
- Increasing involvement of insurance providers and payers in primary prevention
- Reducing primary care physician burnout
References:
- CMS. (2013). National Health Expenditure Projections 2012-2022. Retrieved from http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/proj2012.pdf
- Robert Wood Johnson Foundation. (2011). What are the biggest drivers of cost in U.S. health care? Health Policy Snapshot. Retrieved from http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2011/rwjf71331
- Munro, D. (2014). Annual U.S. Healthcare Spending Hits $3.8 Trillion. Forbes. Retrieved from http://www.forbes.com/sites/danmunro/2014/02/02/annual-u-s-healthcare-spending-hits-3-8-trillion/
- Aetna. (2012). The Facts About Rising Health Care Costs. Retrieved from http://www.aetna.com/health-reform-connection/aetnas-vision/facts-about-costs.html
- Wilson, K. (2013). Health Care Costs 101. California Health Care Almanac. Retrieved from http://www.chcf.org/publications/2013/09/health-care-costs-101
- Luhby, T. (2014). Health care spending growth remains low. CNN Money. Retrieved from http://money.cnn.com/2014/01/06/news/economy/health-care-spending/
- PWC. (2013). Medical cost trend: behind the numbers 2014. Health Research Institute. Retrieved from http://www.pwc.com/en_us/us/health-industries/behind-the-numbers/assets/medical-cost-trend-behind-the-numbers-2014.pdf
- Trends in health care cost growth and the role of the affordable care act. (2013). Retrieved April 09, 2014, from http://www.whitehouse.gov/sites/default/files/docs/healthcostreport_final_noembargo_v2.pdf
- America’s Health Insurance Plans. (2013). Rising Health Care Costs. American Journal of Managed Care. Retrieved from http://www.ahip.org/Issues/Rising-Health-Care-Costs.aspx
- Ogden, C. L., Carroll, M. D., Kit, B. K., & Flegal, K. M. (2014). Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA : The Journal of the American Medical Association, 311(8), 806–14. doi:10.1001/jama.2014.732
- De Vol, R., & Bedroussian, A. (2007). An unhealthy america: the economic burden of chronic disease. Milken Institute. Retrieved from http://www.milkeninstitute.org/pdf/chronic_disease_report.pdf
- Finkelstein, E. A., Trogdon, J. G., Cohen, J. W., & Dietz, W. (2009). Annual medical spending attributable to obesity: payer-and service-specific estimates. Health Affairs (Project Hope), 28(5), w822–31. doi:10.1377/hlthaff.28.5.w822
- Louise B. Russell, “Preventing Chronic Disease: An Important Investment, But Don’t Count On Cost Savings,” Health Affairs 28 (2009): 42–45, doi: 10.1377.
- Cohen JT, Neumann PJ, Weinstein MC. Does preventive care save money? Health economics and the presidential candidates. N Engl J Med 2008;358:661-3.
- Mongan JJ, Ferris TG, Lee TH. Options for slowing the growth of health care costs. N Engl J Med 2008;358:1509-14.
- Goodman Ph.D., J. (2013). Will More Preventive Care Help Reduce Healthcare Costs? | Psychology Today. Psychology Today. Retrieved from http://www.psychologytoday.com/blog/curing-the-healthcare-crisis/201303/will-more-preventive-care-help-reduce-healthcare-costs
- Fruge, D. (2012). Impact of primary care on healthcare cost and population health. Rhode Island Department of Health. Retrieved from http://www.health.ri.gov/publications/literaturereviews/ImpactOfPrimaryCareOnHealthcareCostAnd PopulationHealth.pdf
- Cunningham, July 18, 2006. McCaig L and Nawar E. National Hospital Ambulatory Medical Care Survey: 2004 Emergency Department Summary. National Center for Health Statistics, Advance Data from Vital and Health Statistics, no. 372. June 23, 2006. http://www.cdc.gov/nchs/data/ad/ad372.pdf.
- Hiramoto M.D., J. (2014). Late Diagnosis of PAD in Women Increases Risk. UCSF Heart & Vascular Center News. Retrieved from http://www.ucsfhealth.org/pdf/heart_and_vascular_center_news_spring_2014.pdf
- Woolf, MD, MPH, S., Husten, MD, MPH, C., Lewin, MBA, L., Marks, MD, MPH, J., Fielding, MD, MPH, MBA, J., & Sanchez, MD, MPH, E. (2009). The economic argument for disease prevention: distinguishing between value and savings. National Commission on Prevention Properties. Retrieved from http://www.prevent.org/data/files/initiatives/economicargumentfordiseaseprevention.pdf
- Goodell, MA, S., Cohen, PhD, J., & Nuemann, ScD, P. (2009). Cost savings and cost-effectiveness of clinical preventive care. Robert Wood Johnson Foundation Policy Brief No. 18. Retrieved from https://www.statereforum.org/system/files/preventive_care_brief_final.pdf
- Campbell, W. B., Skidmore, R., Woodcock, J. P., & Baird, R. N. (1985). Detection of early arterial disease: a study using Doppler waveform analysis. Cardiovascular Research, 19(4), 206-211.
- Marks, J. B. (2003). The Daily Walk or the Daily Pill? Clinical Diabetes, 21(2), 51-52.
- Suzuki, T., Kohro, T., Hayashi, D., Yamazaki, T., & Nagai, R. (2012). Frequency and impact of lifestyle modification in patients with coronary artery disease: the Japanese Coronary Artery Disease (JCAD) study. American heart journal, 163(2), 268-73.
- McKee, M. G. (2008). Biofeedback: an overview in the context of heart-brain medicine. Cleveland Clinic journal of medicine, 75 Suppl 2, S31-4.
- Kesselman, P. (2006). Non-Invasive Arterial Vascular Testing Diagnostic Vascular. Podiatry Management.
- Draper, D. (2009). Insights into the Health Care Marketplace: a key to higher quality and low cost growth or a lost opportunity? Center for Studying Health System Change, (3).
- Lakhan, S. E., & Laird, C. (2009). Addressing the primary care physician shortage in an evolving medical workforce. International Archives of Medicine, 2(1), 14. doi:10.1186/1755-7682-2-14
- Rosser, W. W. (2002). The decline of family medicine as a career choice. CMAJ : Canadian Medical Association Journal = Journal de l’Association Medicale Canadienne, 166(11), 1419–20. Retrieved from http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=111215&tool=pmcentrez&rendertype=abstract
- Halbesleben, J. R. B., & Rathert, C. (n.d.). Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Health Care Management Review, 33(1), 29–39. doi:10.1097/01.HMR.0000304493.87898.72
- Dyrbye, L. N., & Shanafelt, T. D. (2011). Physician burnout: a potential threat to successful health care reform. JAMA : The Journal of the American Medical Association, 305(19), 2009–10. doi:10.1001/jama.2011.652
- Sinsky, C. A., Willard-Grace, R., Schutzbank, A. M., Sinsky, T. A., Margolius, D., & Bodenheimer, T. (2013). In search of joy in practice: a report of 23 high-functioning primary care practices. Annals of Family Medicine, 11(3), 272–8. doi:10.1370/afm.1531
- Blue Shield of California. (2005) Physician Performance Measurement Program Report. Retrieved from https://templetondoc.com/wp-content/uploads/2014/04/Scan-1.pdf
- Santamarina, J., Castellanos, M.D., A. (2012) Bi-directional Spectral Doppler Waveform Analysis Used in Reversal of Coronary Artery Disease: A Case Study. Retrieved from https://templetondoc.com/wp-content/uploads/2014/04/Case-Study-Draft-9.pdf
- Santamarina, J., Castellanos, M.D., A. (2013) Vascular Improvement for Performance in Sports. Retrieved from https://templetondoc.com/wp-content/uploads/2014/04/VIPS.pdf
- Castellanos, A. (2006). System for improving vascular systems in humans using biofeedback and network data communication. 20060229506.
- Castellanos, A. (2002). Method and system for improving vascular systems in humans using biofeedback and network data communication. US20020183599 A1.